Advocacy Paper
Coordination is Care
A shared position paper that makes invisible coordination work visible and creates a common language for socio-medical care coordination.
View document →Bachelor Graduation Project · 2026
Designing Visible Care Coordination at Socio-Medical Transitions
Five phases from first observation to tested intervention. Hover over each phase to explore.
Mapping the landscape of integrated care. Understanding the system before entering it.
→ Contextual understanding of fragmented care.
Going into the field. Listening to healthcare professionals, observing coordination in practice.
→ Rich picture of how coordination works and where it breaks down.
Triangulating findings, mapping the system, reframing the challenge from structural to relational.
→ Area of opportunity: coordination as relational practice.
Developing two complementary design interventions through co-design moments and iterative prototyping.
→ Advocacy Paper and Socio-Medical Handover Baton.
Testing interventions with healthcare professionals, gathering feedback, thinking about implementation.
→ Grounded understanding of what the interventions can and cannot do.
The problem is not that care coordination is missing; it is that it remains invisible, poorly understood, and therefore difficult to share.
Care coordination is already happening. Not through formal structures, but through invisible work carried by healthcare professionals, relatives, and volunteers.
Coordination already exists, but it cannot be recognised, discussed, shared, or improved because it remains invisible.
Everyone agrees integrated care is important. But when asked what it actually means in everyday practice, people struggle to answer.
Socio-medical transitions are the moments where information, responsibility and care are most likely to fragment.
Coordination depends on relationships before it depends on structures.
The healthcare system optimises individual actors, but rarely the transfer between them.
What becomes visible can become discussable, recognisable and eventually shareable.
The emergence of SOMEKO creates an opportunity to embed care coordination into existing care pathways rather than adding another isolated service.
The Swiss healthcare system works. But often because people coordinate beyond their formal roles. Each contributes to the same care situation, but still works from a different part of the system. This work is called invisible care coordination.
Patient care does not emerge within a single organisation, but through the interaction of multiple system levels. At the macro level, policies, strategies, and funding structures shape the conditions of care. The meso level consists of regional networks and organisations that enable and coordinate collaboration across services. At the micro level, care takes place in practice—where patients, relatives, and healthcare professionals navigate everyday decisions and transitions.
The quality of care coordination depends on the interaction between all three levels. Care coordination therefore does not happen in one specific place, but in the handovers between levels—where information, responsibility, and decision-making are passed on.
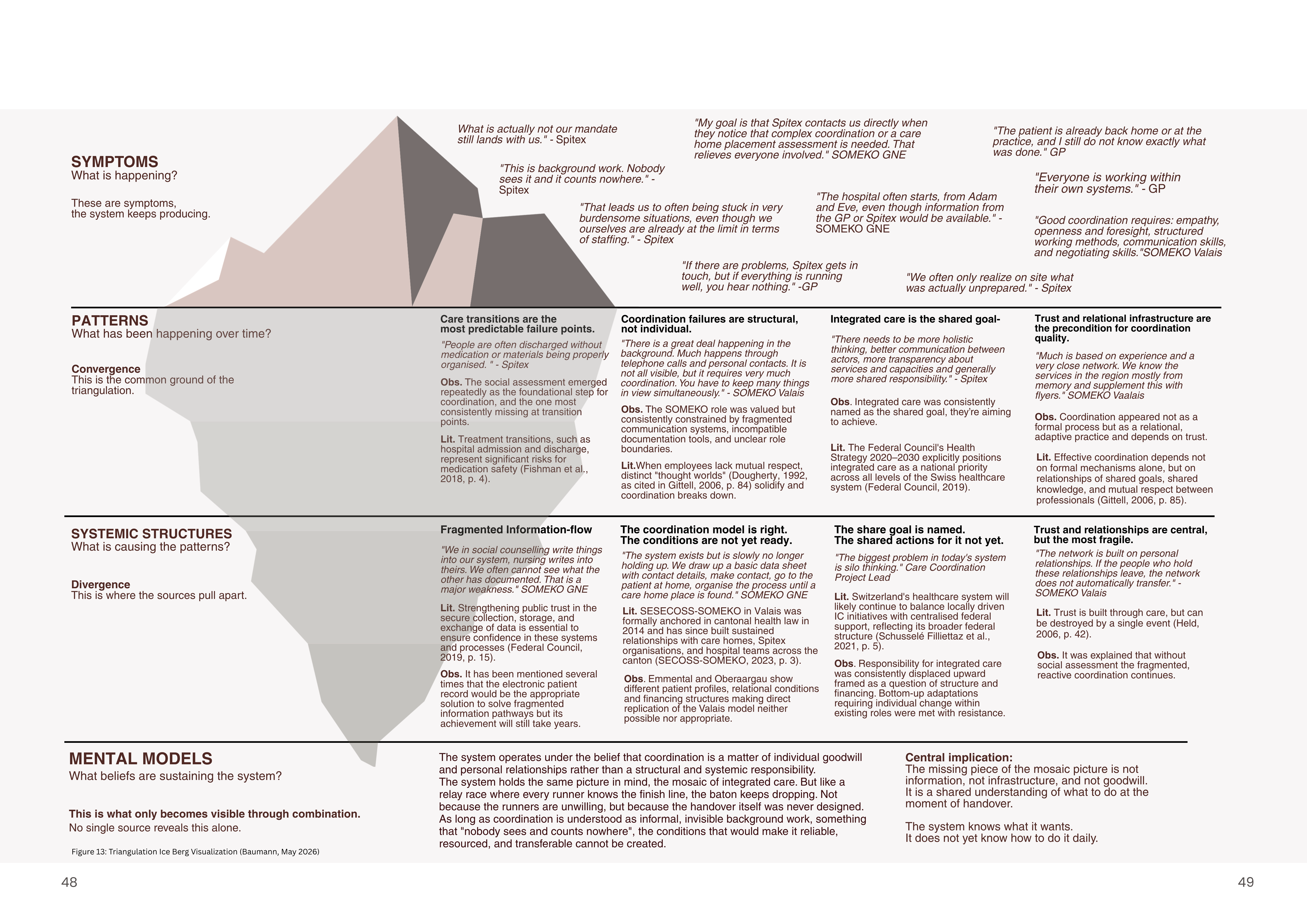
The surface shows what is formally recognised. Below the waterline lives the work that keeps care together — invisible, unprotected, and unacknowledged. This triangulation map brings together field observations, expert interviews, and literature to make that invisible layer visible.
Coordination as an administrative or structural problem.
Coordination as relational care work.
Coordination is not an extra service added onto care.
The project does not claim to solve fragmentation by giving a tool or a product that strictly needs to be used by everyone. Instead it creates conditions for care coordination to become something people can recognise, discuss, and deliberately design for — working at the level of interactions, communication and handovers.
Shared language for coordination
Visible coordination work
Clearer handovers at transitions
Reduced repetition of patient information
Stronger relational coordination
Support for SOMEKO's recognition
Bridge between everyday practice and system-level transformation
Three artefacts that make care coordination visible, structured, and shareable.
A shared position paper that makes invisible coordination work visible and creates a common language for socio-medical care coordination.
View document →A system-independent handover tool that travels across transitions and helps ensure that what one actor knows, the next one receives.
A supporting document that enables information to be shared safely, legally, and ethically across organisations.
View document →Do you work in healthcare, coordination, or system design? Have thoughts on the interventions, the reframing, or the approach? I would love to hear from you.
rosanabaumann@gmail.com